 GGC Paediatric Guidelines
GGC Paediatric Guidelines
Bronchoalveolar lavage (BAL) is an invasive procedure used to collect samples from the lower respiratory tract. BAL can be performed via bronchoscopic and non-bronchoscopic (also known as ‘blind’) methods. Samples obtained can be tested for microbiology and virology to identify pathogens which may not be detected with endotracheal (ET) or nasopharyngeal aspirates alone. Blind BAL is a relatively quick and easy procedure, does not require technical expertise in bronchoscopy and can be performed where the ET tube is too small for a bronchoscope.
Blind bronchoalveolar lavage (BAL) guideline - neonates
Warning
Objectives
To support the increased use of BAL within the neonatal unit for diagnosis of bacterial and viral pneumonias.
Audience
This guidance is applicable to all Medical staff, Advanced Neonatal Nurse Practitioners and Nursing staff working in the neonatal units in NHS Greater Glasgow & Clyde.
- Sterile drape
- Sterile gloves and plastic apron
- One tracheal suction trap
- One universal container
- 5ml syringe
- Sterile green needle
- 10ml normal saline
- Argyle suction catheter
- Three-way tap
- Male-male connector
- Luer lock suction connector
Trolley set up shown in Figure 1.

Figure 1: Equipment laid out on sterile field
(1) Argyle suction catheter, (2) Three-way tap, (3) Male-male connector, (4) Luer lock suction connector, (5) 10ml normal saline vial, (6) green needle, (7) 5ml syringe, (8) tracheal suction trap with white cap
- Allocate roles:
- One person is responsible for inserting and withdrawing the suction catheter from the ET tube under sterile technique.
- One person operates the three-way tap and administers the saline instillation.
- One person to monitor patient during procedure.
- Ensure the patient is stable and well oxygenated prior to commencing the procedure.
- Prepare the equipment at the cotside:
- Open all the equipment onto the sterile field
- Wash hands, put on apron and sterile gloves
- Draw up 1-2ml normal saline into a 5ml syringe with a 3ml “air chaser”
- 1ml if <32 weeks gestation
- 2ml if ≥32 weeks gestation
- Assemble equipment as per Figure 2
- Connect the Argyle suction catheter tube to the three-way tap
- Connect the male-male connector to the three-way tap on the opposite port to the Argyle suction catheter
- Connect the Luer lock suction connector to the male connector
- Connect the Luer lock suction connector to the inlet of the tracheal suction trap
- Connect the suction tubing to the suction end of the tracheal suction trap, ensuring the three-way tap is off to suction (Figure 3)
- Connect the syringe with saline and air chaser to the third port of the three-way tap
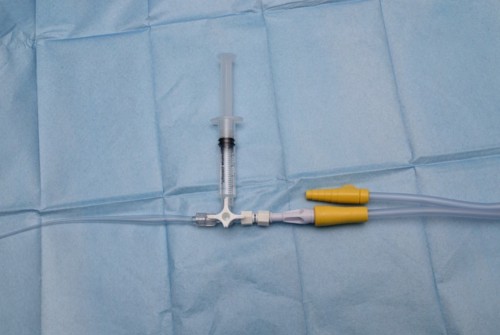
Figure 2: Equipment assembled
 |
Ensure the syringe with saline and the tracheal suction trap are held vertically throughout. |
 |
Disconnect the ET tube from the ventilator and advance the Argyle suction catheter gently into the ET tube into the lower airways until resistance is met. |
 |
Stop once the suction catheter is in place, alert other operator. |
 |
Administer the saline with air chaser, then count to 3 seconds to allow dwell time in lower airways. |
 |
Without moving the Argyle suction catheter, turn the three-way tap so it is open to the suction (Figure 4) and slowly pull the Argyle suction catheter back (by maximum 2cm) then turn the three-way tap back off to the suction (Figure 3). This ensures only bronchial sample is collected. |
 |
Remove the Argyle suction catheter from the ET tube and connect the ET tube back to the ventilator. |
 |
Due to the small volume of saline instilled, most of the sample will be within the Argyle suction catheter with minimal sample in the tracheal trap. |
 |
Once the Argyle suction catheter is removed from the ET tube, insert it into a vial of sterile saline and turn the three-way tap on to the Argyle suction catheter (Figure 4). This will encourage the sample to move from the suction catheter into the tracheal trap container. A suggested sample amount is 5ml. |
 |
|
 |
|
Figure 3: Three-way tap off to suction |
Figure 4: Three-way tap on to suction |


- Bronchial sample appears cloudy or milky with white casts (Figure 5).

Figure 5: Bronchial sample with white casts
- Carefully decant half of the sample into a universal container, so two separate samples can be sent for testing.
- Ensure container caps are firmly secured.
One sample is sent for Virology and the other for Microbiology. Both samples are to be sent in white top (universal contaniers) only. Request samples via TrakCare as below:
- Virology: search Labs for “BAL screen (PCP/CMV/Resp virus/Mycoplasma pneumonia)”
- Once selected, choose specimen type “Blind Br.Alveol.Lav – Vir”
- Figure 6 and 7
- Microbiology: search Labs for “General Bacterial Culture (not TB)”
- Once selected, choose specimen type “Blind Br.Alveol.Lav – Bact”
- Figure 8
- Complete the request with the patient’s clinical details

Figure 6: Blind BAL Virology request on TrakCare

Figure 7: Blind BAL Virology request on TrakCare

Figure 8: Blind BAL Microbiology request on TrakCare
Document with the Blind BAL procedure sticker in the patient’s notes.
Blind BAL procedure sticker