The majority of babies admitted to the NNU with low saturations following pulse oximetry screening will not have underlying cardiac pathology. More than half will have a respiratory cause, around 20% will have a transitional circulation and only 6-8% will have a cardiac cause. Therefore, investigations and management of the baby will be dependent on the differential diagnosis.
a. Differential Diagnosis:
In studies assessing POS, the most common differential diagnoses were:
- Congenital pneumonia
- Meconium aspiration
- PPHN
- Pneumothorax
- Culture negative sepsis
- GBS sepsis
Cardiac causes included:
- Transposition of the great arteries (TGA)
- Critical pulmonary stenosis
- Interrupted aortic arch (IAA)
- Total anomalous pulmonary venous connection (TAPVC)
- Hypoplastic left heart syndrome (HLHS)
The benefit from early detection of CCHD is predominantly the prevention of acute collapse and death. Therefore, the following lesions are key targets for pulse oximetry screening:
- Hypoplastic left heart / single ventricle
- Pulmonary atresia with intact ventricular septum
- TGA
- IAA
- TAPVC
- Coarctation of the aorta
- Aortic stenosis
- Tetralogy of Fallot
b. Initial Investigations and Management in the NNU
The investigations and management will be dependent on each individual case. The aim being to exclude or confirm cardiac or other pathology.
Investigations /Management to consider:
- Maternal History
- Risk factors for sepsis
- Meconium staining
- Top to Toes examination, oxygen/respiratory support and observe response
- Blood gas
- CXR
- Antibiotics
- Continuous pre/post ductal saturations
- Echo if no other explanation for persistent hypoxaemia
A baby on the red pathway does not automatically warrant an echocardiogram.
c. When to request an echocardiogram
The majority of babies admitted to the NNU via the red pathway of POS will not have cardiac pathology, therefore routine echocardiography in all babies is not advised.
Requesting of an echocardiogram should be a consultant decision.
There are 2 scenarios when an echocardiogram is advised:
- Baby has no other reasonable explanation for their hypoxia (after investigation)
- There are other indicators suggestive of cardiac lesion, such as a murmur or poor perfusion/weak pulses.
The urgency with which the echocardiogram is performed is dependent on the clinical condition of the baby.
In RHC cardiology have agreed that an echocardiogram can be requested without discussion with the on-call cardiology consultant in the event of a NNU admission for a red POS (baby not unwell and looking like delayed transition/sepsis).
In PRM/RAH this would be dependent on the team available and anticipation of likely transfer to RHC. The attending consultant neonatologist may conduct an initial echo to confirm cardiac aetiology. They can then consult with the cardiology team at RHC, receiving neonatal consultant at RHC and ScotSTAR in the event a transfer is required.
Alternatively, the on-call cardiology team at RHC can be directly consulted for advice in relation to arranging an echocardiogram.
The unwell baby who needs an echocardiogram:
If the baby is becoming critically unwell with suspected congenital heart disease, there should be urgent discussion with on-call cardiology, consideration of a prostin infusion and, for those babies out-with RHC, discussions with ScotSTAR regarding potential transfer to RHC for further assessment.
d. Performing POS on the NNU
In babies admitted to the NNU POS should be performed very shortly before discharge from NNU.
This includes all babies who were born very preterm, as well as those who are late preterm or term who are admitted from labour ward or admitted before 6 hours of life.
Eligible Babies transferred back to the post-natal ward should have POS completed prior to transfer.
It is the responsibility of the neonatal unit medical team to ensure POS has been undertaken for EVERY baby prior to discharge.
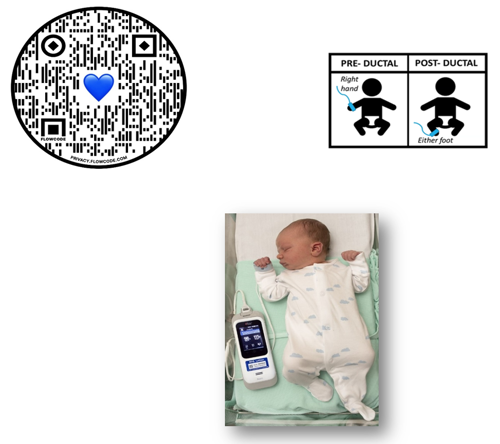
Measure pre and post ductal saturations as previously discussed and assign the baby to a pathway (green, amber or red).
e. Documentation
Document the POS in the maternity badger. How we document this screening is vital.
It must be documented in Badger in Oxygen Saturations (even if done as part of the NIPE)

The Pathway assigned must then be documented as a clinical alert in the baby records e.g. Pulse Ox Green, Pulse Ox Amber or Pulse Ox Red (see below).

When the practitioner then clicks on the Oxygen Saturations box it should look like this. The preductal and post ductal sats must be documented on this form.


When Neonatal staff come to review an infant on the Amber or Red Pathway, they should document their plan in their Specialist Review (see below)

 GGC Paediatric Guidelines
GGC Paediatric Guidelines