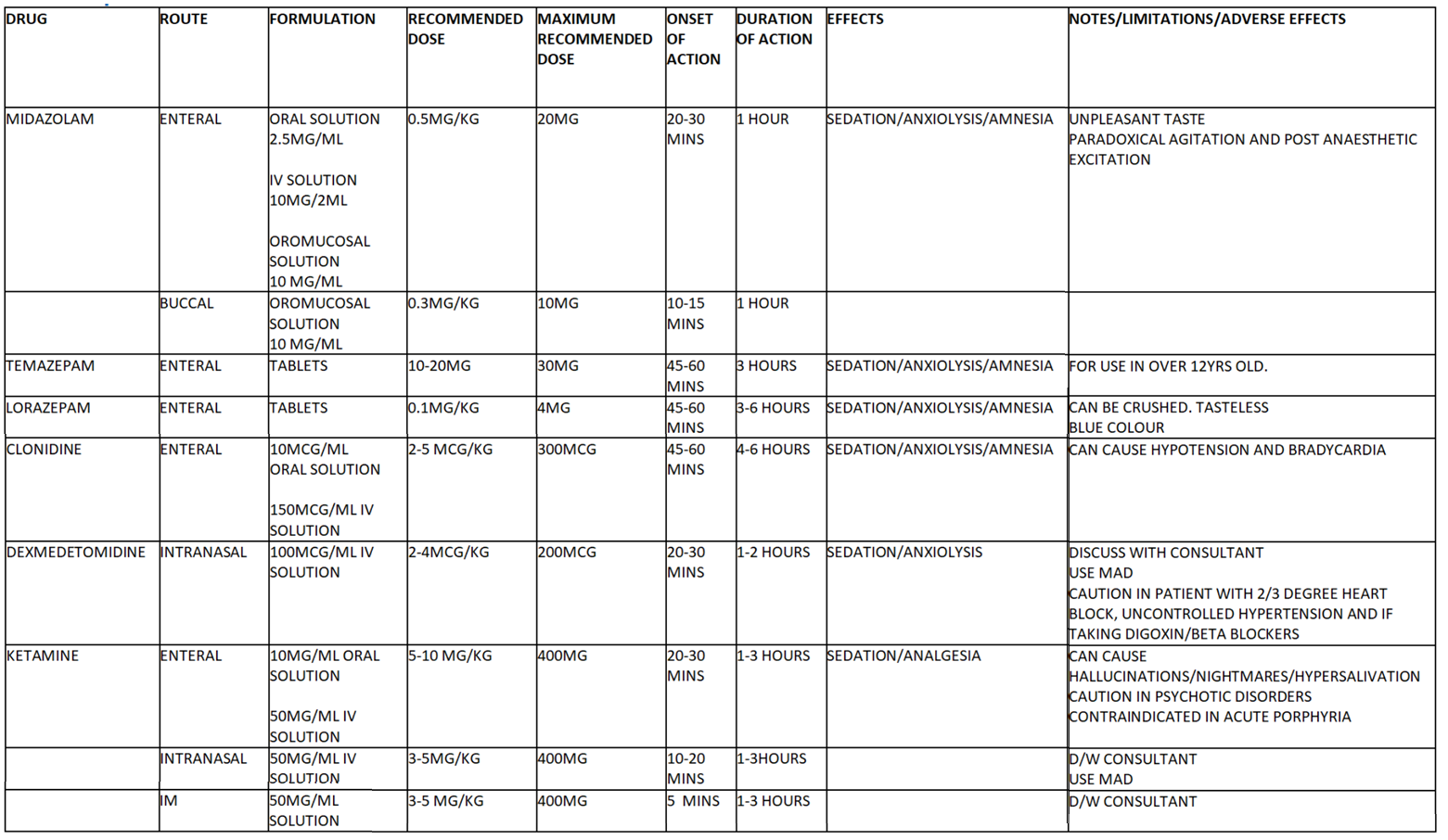
The above medication table is not exhaustive but covers the commonly seen sedative premedications.[2]
The anaesthetist may use a combination of sedative premedication drugs to achieve the desired level of sedation, within an appropriate time frame.
Please consider onset time when prescribing 2 or more agents. EG if prescribing clonidine and midazolam, consider giving clonidine first and midazolam after 20 minutes so both reach effect at same time. Staggering may also make midazolam more palatable.
Patients with autism: frequently patients with autism experience post procedure agitation if given midazolam alone. Please co prescribe with clonidine or administer clonidine in theatre to help counter act the agitation. Ketamine/clonidine combination works well.
The recommended doses/kg and maximum doses can be exceeded, but this is the responsibility of the prescribing anaesthetist. This must be discussed with a consultant anaesthetist and should be clearly documented and communicated with the responsible nurse.
Care should be taken when prescribing in the overweight child, with consideration made regarding ideal body weight vs. actual body weight.
The administration of IM ketamine should performed by an anaesthetist in an environment in which it is safe to do so. It should contain appropriate monitoring and anaesthetic equipment. The administrating anaesthetist must have sight of the child at all times.
Repeat premedication doses may be required, especially if the child has not taken the original dose effectively. This should be written up by the anaesthetist and administered with the appropriate monitoring as necessary.
 GGC Paediatric Guidelines
GGC Paediatric Guidelines