
Recognition and management of maltreatment in infants (children under the age of 1)
exp date isn't null, but text field is
Objectives
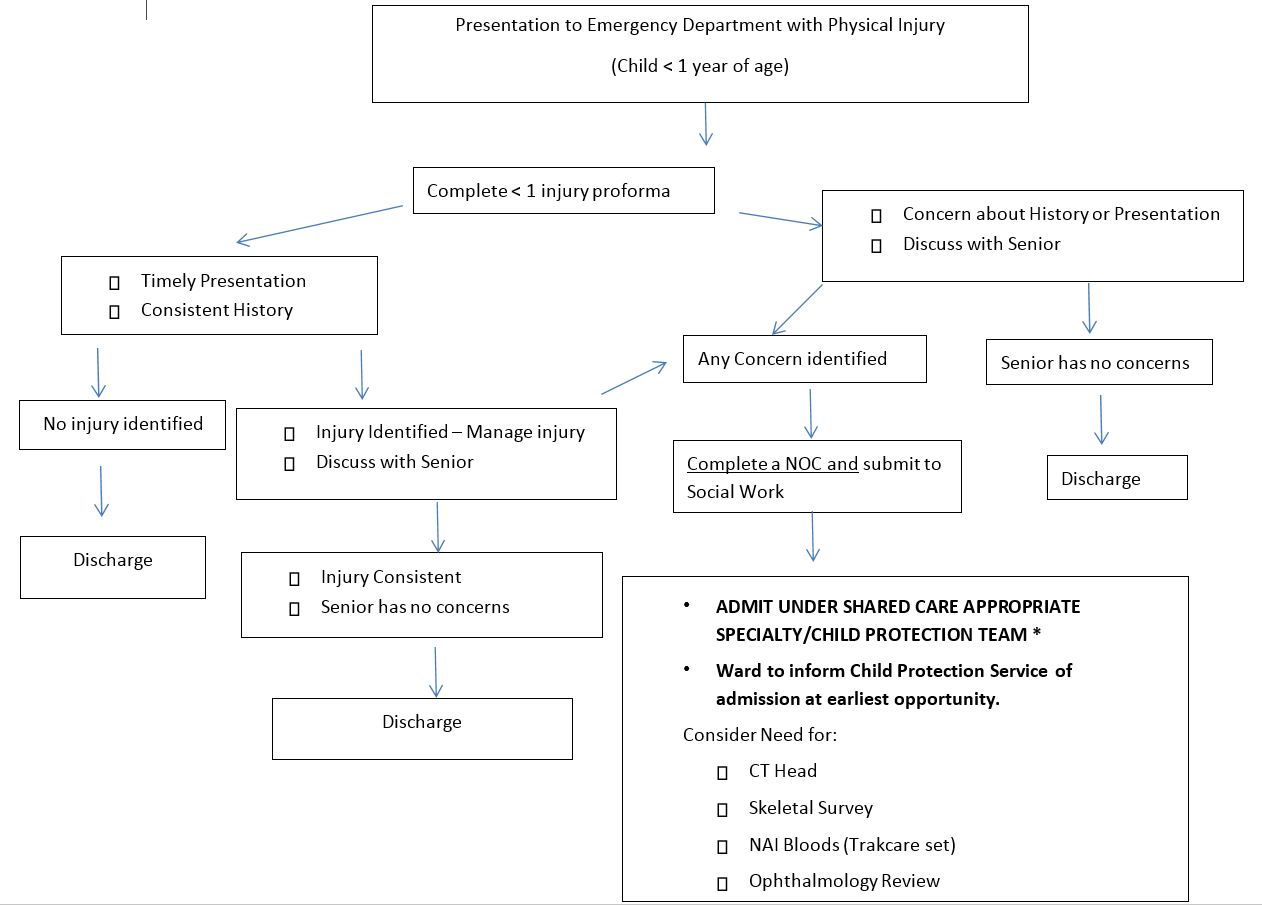
This document aims to assist clinicians in the management of children who present with an injury under the age of 1 year and where there are concerns about their welfare and protection.
This should be used in conjunction with the “Under 1 injury proforma”
This guideline should be used in conjunction with National Guidance National Guidance for Child Protection in Scotland 2014
There are also good practice recommendations from the RCPCH Child Protection Companion section 9: RecRecognitognition of physical abuse | RCPCH
Scope
This guidance is targeted particularly for Hospital-based practitioners, but may also be a useful guide for other settings, disciplines and agencies regarding identification of infants presenting in the acute setting.
Hospital-based clinicians have a responsibility to identify and respond to children who are at risk of or suffering child abuse and neglect. Clinicians have a duty to work in partnership with the other statutory agencies (Social work and Police) in the identification and investigation of concerns regarding child protection.
Whenever an infant presents with an injury it is essential that a detailed history regarding the mechanism of injury be documented. Whenever possible this should be from an eye witness. This should include details of the child’s development. Infants should be examined top to toe to ensure that no further injuries are present. This is all detailed in the accompanying Under 1 proforma. There is a low threshold for infants under 1 with such injuries being admitted. There may also be sufficient concern to warrant further investigation if alerting features such as:
- Lack of parental supervision
- Drug/alcohol misuse
- Parental mental health problem
- Domestic Abuse
- Previous concerning presentations to other professionals
- Signs suggestive of neglect/emotional abuse
- Care must be taken regarding assessment siblings especially twins
- Are present
This allows other investigations such as skeletal survey, head CT and ophthalmological assessment. If clinical decision is not to proceed to admission the reasons for this should be clearly documented in the notes.
If practitioners have concerns about an under 1, then a urgent referral by telephone should be made to social work services (see table below) and you should request a child protection investigation. A Notification of Concern form (previously known as Shared Referral Form) via Clinical Portal E-forms should also be completed for all cases.
If required:
Advice can always be sought on a 24/7 basis from the child protection service – See table below:
|
|
RHC/GRI |
RAH |
IRH |
|
Child Protection Service Weekdays – 9am to 5pm |
0141 451 6605 |
As RHC |
As RHC |
|
Child Protection Medical Paediatrician on call Weekdays 5pm to 9am/weekends/ public holidays |
0141 201 0000 (switchboard) |
As RHC |
As RHC |
|
Child Protection Consultant on call 24/7 Complex physical injury/sexual abuse cases |
0141 201 0000 (switchboard) |
As RHC |
As RHC |
There are many signs and symptoms most of which are non-specific. For further information regarding these please refer to the following document: NICE Guidance CG89 - Child maltreatment - When to suspect maltreatment in under 16s
In addition there is the RCPCH Companion for RCPCH members:-
RCPCH Child Protection Companion (Hard copy of this can be obtained directly from the RCPCH)
Non ambulant children are less likely to sustain an injury than an ambulant child and this is particularly true with fractures. There are also areas on the body much less likely to be affected by bruising. Particular care must be taken when dealing with a non-ambulant child with any sort of injury. For further information please refer to the RCPCH Child Protection Companion for the injury types in more detail.
RCPCH members can access the Child Protection Companion via the following link:- RCPCH Child Protection Companion
- Fractures - 9.5.1 – 9.5.52
- Bruising patterns - 9.3.18 – 9.3.19
- Burns - Chapter 9.1 – 9.9.24 (Burns and scalds)
- Bites – 9.4
- Intra-abdominal injuries:- 9.8 (Abusive abdominal and visceral injuries)
- Head injuries - 6 (Abusive head trauma (AHT))
For non RCPCH members, you can access more information regarding injury types using the link: https://www.nice.org.uk/guidance/cg89/resources/childmaltreatment-when-to- suspect-maltreatment-in-under-16s-975697287109. These can be found in Section 1.1 from Page 12 to 15.
If the child is admitted because of concerns regarding child abuse and /or neglect, the admitting team should always share care with the Child Protection Service in order to complete the interagency child protection investigation. Part of this process includes an Initial Referral Discussion with the Police and Social Work, and a child protection case discussion/conference prior to the child’s discharge from hospital. This will be convened, chaired and minuted by Social Work department.
NOTES:
All child protection concerns should be discussed with the senior on for your department/specialty prior to escalating concern or discharging the patient.
(In RHC this should be the ED consultant if present in the building, and the on-call medical registrar out with these times). In Clyde this should be the EM consultant if present or EM middle grade if not.
These pathways are for guidance only, non-verbal children of any age and children with special needs are more vulnerable and therefore may require further investigation.
If the child requires admission and there are child protection concerns, admit under shared care appropriate specialty and the child protection service.
All specialities will share care with the child protection service if child protection concerns have been identified. They will remain involved for the care of the injury/ medical care of the child.
In the RHC children requiring admission should be admitted straight to ward as per CDU admission flow pathways (they are unlikely to go home within 24 hours and will require significant input).
Please note if following the under 1 proforma and admitting a twin for child protection concerns, BOTH twins require to be admitted and investigated.
Last reviewed: 30 April 2018
Next review: 30 July 2019
Author(s): Wendy Mitchell, Chief Nurse & Head of Child Protection
Approved By: Child Protection Forum