
First afebrile seizure, management
exp date isn't null, but text field is
Objectives
Guidance on the assessment, investigation and management of children with their first afebrile seizure.
Scope
Who is afebrile?
Temp below 38 degrees
If history and examination are suggestive of febrile seizure, the patient should be treated as such even if temp below 38 degrees
Are they still fitting? Have obvious neurological deficit/abnormality?
This guideline is aimed at those children who have fully recovered at time of presentation to ED. If still fitting, follow APLS guidelines on management of seizures. If depressed level of consciousness follow standard ABC approach
TEST BLOOD SUGAR (NEAR PATIENT TESTING) IN ANY CHILD WHO IS FITTING OR WHO HAS A REDUCED LEVEL OF CONSCIOUSNESS AT TIME OF PRESENTATION
For further information see “The management of a child with a decreased conscious level” in RHSC Emergency Medicine Clinical Guidelines.
SEEK SENIOR INVOLVEMENT IN PROLONGED SEIZURE AND THOSE WHO DO NOT RECOVER FULLY
Audience
Medical and nursing staff working in the Emergency Department, Clinical Decisions Unit and acute admissions unit.
November 2023: This guidance is currently under review as it has gone beyond the standard review date. It reflects best practice at the time of authorship / last review and remains safe for use. If there are any concerns regarding the content then please consult with senior clinical staff to confirm.
A first seizure of any kind is frightening to those who witness it. Parents have often thought that their child was going to die, and this anxiety must be understood, and if appropriate, allayed. The child may appear absolutely well by the time they arrive in the department.
TEST BLOOD SUGAR (NEAR PATIENT TESTING) IN ANY CHILD WHO IS FITTING OR WHO HAS A REDUCED LEVEL OF CONSCIOUSNESS AT TIME OF PRESENTATION
For further information see “The management of a child with a decreased conscious level” in RHC Emergency Medicine Clinical Guidelines.
SEEK SENIOR INVOLVEMENT IN PROLONGED SEIZURE AND THOSE WHO DO NOT RECOVER FULLY.
In a significant proportion of children presenting with a first afebrile seizure no diagnosis is found.
Differential diagnoses
1st presentation epilepsy
Acute symptomatic seizure i.e. related to:
- Intracranial infection
- Ingestion
- Trauma
- Tumour
- Intracranial haemorrhage
- Hypertension
- Hydrocephalus
- Metabolic (low glucose/ calcium/sodium etc)
In children under 3/12 in addition to the above the following diagnoses are considered-
- Hypoxic Ischaemic Encephalopathy (from birth)
- congenital infection
- Fifth day fits
- Drug Withdrawal
- Pyridoxine dependancy
Other important differentials
Convulsive syncope:
- Reflex anoxic seizures
- Vasovagal seizure
- Arrythmias e.g. long QT syndrome
- Suffocation
- Psychogenic seizures
- Due to the anxiety attending seizure activity accurate timescales can be difficult to ascertain. It is useful to have a parent re-live the event that they witnessed, talking through in real time what they saw. This tends to give a more accurate reflection of timings.
- What was the child doing, what happened just before the seizure started?
- Were there any symptoms suggestive of aura? If so, what were they?
- What was the sequence and timing of events?
- Seizure onset and offset? Gradual or sudden?
- What was the child like after the seizure and for how long?
- Was there:
- Awareness during event?
- Unresponsiveness?
- Staring?
- Open or closed eyes?
- Eyelid flutter?
- Eyeball jerking or deviation?
- Facial twitching?
- Body stiffness?
- Chaotic jerking of limbs?
- Rhythmic jerking of limbs?
- Pallor or cyanosis?
- Respiratory effort?
- Any relevant family history of seizures?
Record a detailed chronological history including any focal signs +/- secondary generalised seizure.
Ensure full neurological examination including : -
- level of consciousness
- gait/ cerebellar signs
- fundoscopy if possible
- All children should have their blood pressure checked as part of their routine examination, in this case to exclude systemic hypertension as a rare but important cause of a seizure.
- ECG: children with convulsive seizures may have syncope, including cardiogenic syncope, such as prolonged QT syndrome. ECG with calculation of QTc interval should be calculated on all children presenting with convulsive seizure.
- Age < 1year
- GCS < 15 one hour after seizure
- Signs of raised intracranial pressure, papilloedema, tense fontanelle.
- Meningism
- Signs of respiratory aspiration
- Complex seizure, i.e. prolonged (>15mins), focal or recurrent
- Parents feeling unhappy to take child home following a full discussion.
- In a fully recovered child who you are planning to discharge home. It is not necessary to routinely check a full blood count, urea and electrolytes, calcium or magnesium following a first afebrile seizure or a recurrent seizure, unless history or examination features suggest otherwise.
- If child completely recovered with normal BP and ECG they may be discharged home after parental counselling.
- When counseling parents it is useful to give some indication about the number of children who suffer from a single seizure. Around 1% of children will have an afebrile seizure by the age of 16 and about 50% of those that do will have a recurrence.
1st Seizure clinic referral guidelines
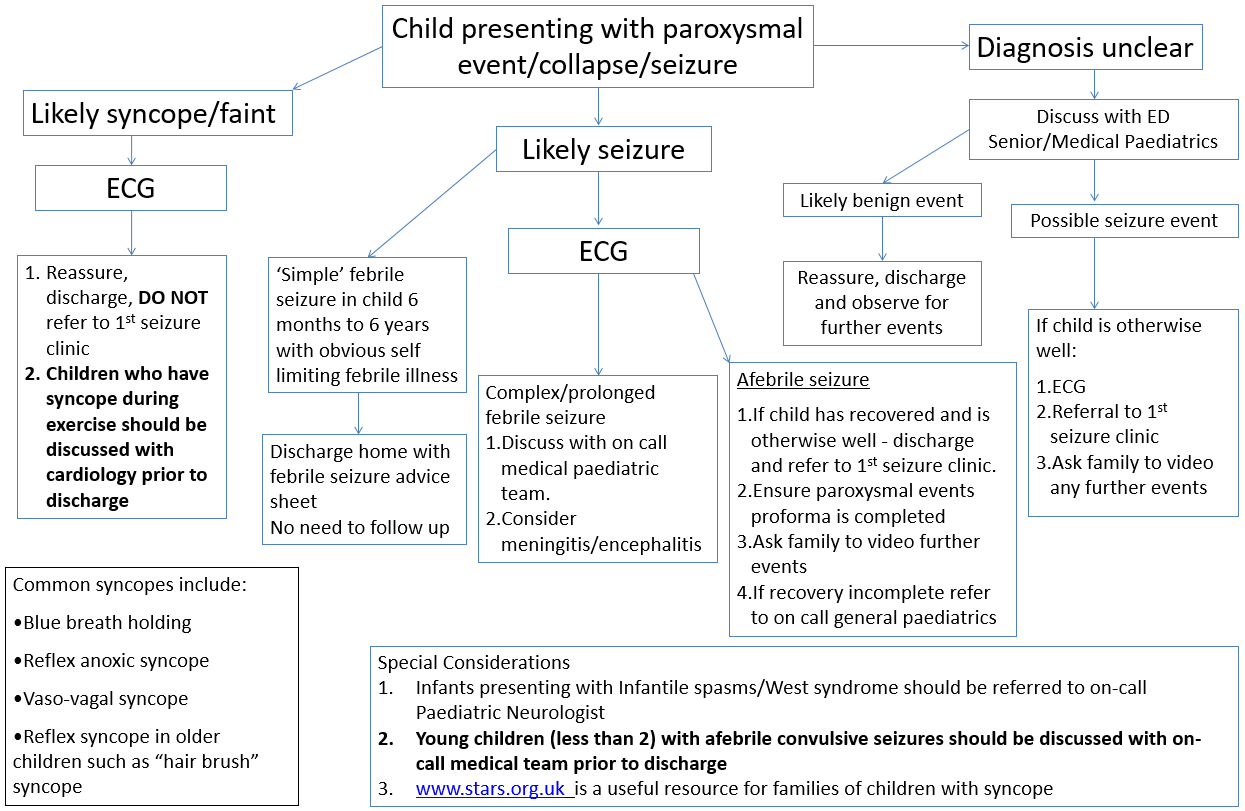
- All children who have had a first afebrile seizure should be referred to General Paediatrics as per 1st seizure clinic referral guide. Please circle General Paediatrics area on the referral appointment sheet (pink sheet) – no dictated letter required for this patient cohort but all clinical details should be completed on the ‘Paroxysmal Events Proforma’.
- All children being discharged from the ED should be given advice on what to do in the event of a further seizure, including indications for calling ambulance / return to ED. Please provide the ‘Patient Information after a possible seizure’ leaflet.
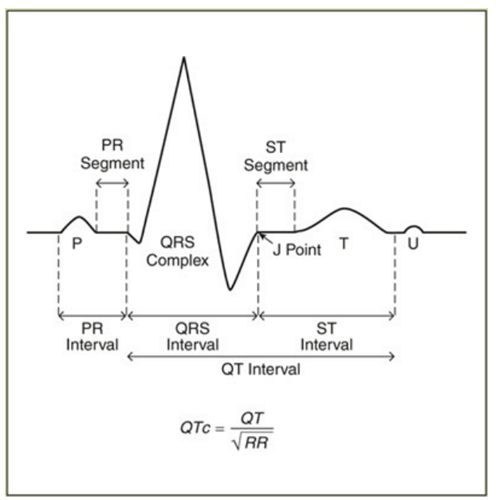
Here's how to calculate the QTc using Bazett's formula:
- Measure the QT interval, choosing a lead in which the T wave is clearly defined. Count the number of small boxes between the beginning of the Q wave and the end of the T wave and multiply by 0.04 for the time in seconds. Write this number down.
- Don't include U waves (discrete waves that appear after the T wave has returned to baseline) as part of the QT interval.
- Measure the R-R interval by counting the number of small boxes between the R wave of the complex you measured the QT time on, and the preceding R wave. Multiply by 0.04 and record the number in seconds.
- Enter the measurement of the R-R interval into your calculator and press the square root button. Write this number down.
- Divide the QT interval by the square root of the R-R interval to obtain the QTc.
- NORMAL QTc <0.44. If the child has a longer QTc than this discuss with senior/cardiology
SIGN 81: Diagnoses and Management of Epilepsies in Children and Young Adults.(2005) [WITHDRAWN]
NICE CG137: Epilepsies: diagnosis & management. (2016)
Paediatric Accident and Emergency Research Group: Seizure - An evidence based guideline for the management of children presenting post seizure (2004)
Last reviewed: 23 October 2018
Next review: 31 October 2024
Author(s): S Foster, V Choudhery
Approved By: Clinical Effectiveness
Reviewer Name(s): ED Guidelines Group
Document Id: 130