 GGC Paediatric Guidelines
GGC Paediatric Guidelines
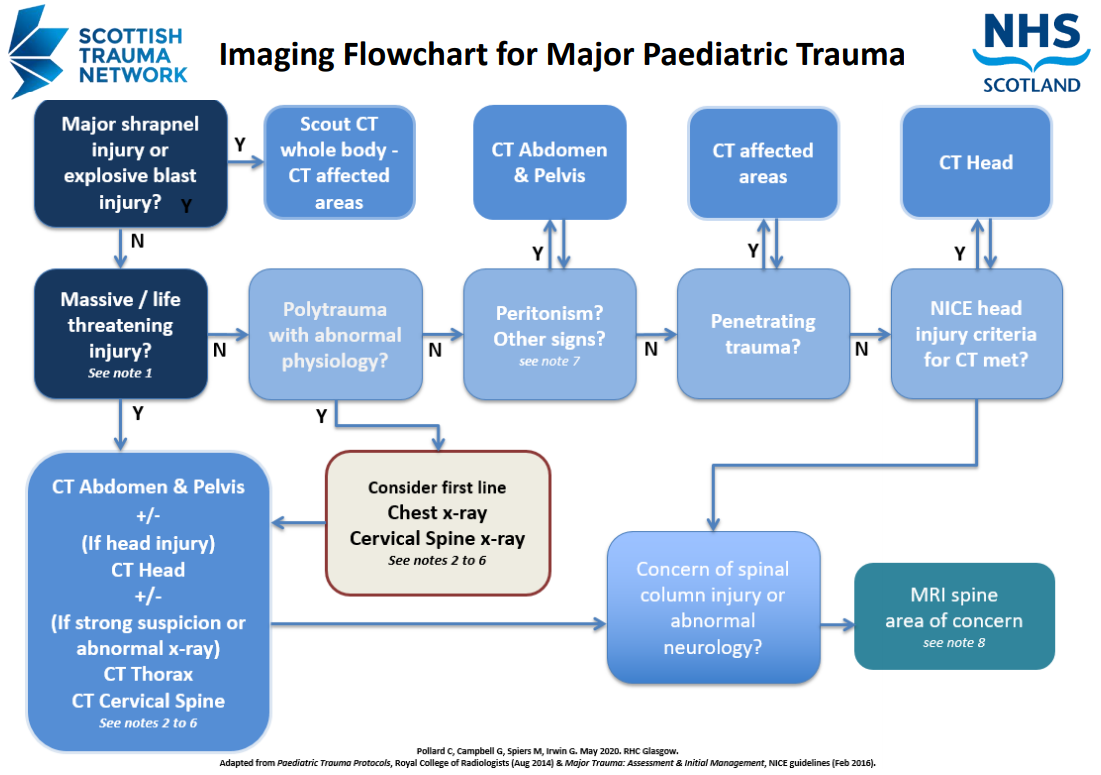
Children have different injury patterns to adults so the imaging strategies are also different. Each child should be imaged on a individualised basis.
There is no place for routine ‘whole body’ or ‘pan scan’ imaging in children, who are considerably more radiation sensitive. There is no role for routine screening pelvis radiographs. Trauma imaging in children should be targeted and selective. This guidance should always be used alongside clinical
judgment.
- If decision is definitely for CT, then do not delay by performing radiographs.
- Pneumothorax will be detected on the uppermost slices of abdominal CT, even if missed on CXR.
- Thoracic vascular injury and aortic syndromes are rare in children.
- Cervical spine fracture is rare in children. Radiation dose to the thyroid is 90-200 fold higher than x-rays and CT will not detect major ligamentous
or cord injury. - NICE guidelines recommend MRI first line for suspected cervical column injury or abnormal neurology. X-rays are second line if MRI not indicated.
Particularly avoid CT in <5 year olds if possible. - CT identifies bony but not ligamentous injuries, and does not ‘clear the neck’. MRI usually performed in-hours.
- Abdominal :
- ecchymosis
- tenderness
- distension
- PR or NG blood
- lap belt injury
- Consider including MRI sagittal stir sequence whole spine for non contiguous injury
