
Congenital syphilis : management of babies born to mothers with syphilis infection
exp date isn't null, but text field is
Audience
This document is applicable to all medical, nursing and midwifery staff caring for the newborn. It should be used with reference to the relevant pharmacy monographs.
Syphilis is caused by the spirochaete Treponema pallidum. It affects a large number of pregnant women worldwide but is now rare in the UK with 50 – 60 cases of syphilis diagnosed in pregnant women each year. Since 2000, the incidence of syphilis in the Scottish population has been increasing with specific outbreaks reported in some Board areas among young heterosexuals, with obvious implications for syphilis in pregnancy. Less than 5 diagnoses of infectious syphilis in pregnancy are diagnosed in Scotland each year and due to a combination of antenatal screening and treatment, congenital syphilis is extremely rare in Scotland. However, in England and Wales there were 7 cases in 2016/17. Congenital syphilis may also present in babies and children recently arrived in the UK where mothers did not undergo adequate antenatal care. Congenital syphilis can be divided into early (<2 years) and late disease (>2 years).
Box 1- Local Arrangements for GUM Advice
|
Greater Glasgow & Clyde - Sandyford Professional Helpline on 0141 211 8646. |
Represents active infection and inflammation. Its main features are low birth weight, rhinitis, snuffles, adenopathy, hepatosplenomegaly, bone abnormalities (periostitis, osteitits, and osteochondritis), hepatitis, anaemia, hydrops and meningitis. However, 2/3 of infected infants will be asymptomatic at birth.
This represents the response to early infection and chronic inflammation. Affected children may have a typical appearance including frontal bossing, saddle nose, short maxilla, high palate, and Hutchinson’s triad (interstitial keratitis, peg shaped incisors, and 8th nerve deafness). These features are not present at birth and some features may only become apparent in early adolescence. Late syphilis can be avoided by correct management of early disease. The likelihood of the infant being affected depends on the staging of maternal infection. The majority of adverse outcomes occur in those with no antenatal screening performed or inadequate maternal treatment. Untreated primary or secondary maternal syphilis carries almost a 100% risk of the fetus being affected, with stillbirth or neonatal death in 40%. Early latent syphilis (defined as within 2 years of onset of infection) carries a risk of fetal infection of approximately 40% and a mortality of around 20%. Late latent (> 2 years from infection) syphilis results in an affected fetus in 10% of cases with a mortality similar to unaffected pregnancies. Note approximately half of all neonates with congenital syphilis are normal on initial examination
Routine antenatal screening for infectious diseases includes tests for syphilis, along with HIV and Hepatitis B. Most cases of maternal syphilis are detected this way. Particular attention must be paid when managing neonates born to mothers who have booked late or present with no antenatal care to ensure all necessary tests are taken and acted upon.
Syphilis screening in pregnancy in NHSGGC is done with an automated enzyme immunoassay (EIA) (Abbott Architect). Around 25% of initial screen-positive EIAs in NHSGGC are actually false positives due to the low prevalence of real infection, with approximately 50% representing previously treated infection. Supplementary testing is undertaken for all positive EIAs and will include:
- RPR: (Rapid Plasma Reagin test) non-treponemal (indirect) antibodies. This test detects biomarkers given off by cells damaged by the syphilis spirochaete. This reflects current disease activity and falls in response to adequate treatment
- TP Syphilis IgM (EIA): This is a direct antibody to the syphilis spirochate. This is positive in early infection and falls slowly (>2years). It does not cross the placenta.
- TPPA: (Treponema Pallidum Particle Agglutination test) a specific treponemal antibody which confirms the EIA is genuine. The exact titre doesn’t really matter.
- InnoLIA Blot test: useful where the markers are discrepant, Needs specialist interpretation
- Syphilis PCR: may be positive from lesions of early syphilis (genital ulcers, mucous patches, condylomata lata)
It is important to determine the stage of maternal illness as this gives an assessment of the risk to the fetus as outlined above. The maternal staging should be assessed by a Consultant Physician in Sexual Health and HIV. All maternal positive results in NHSGGC are forwarded to the Sandyford Failsafe team. The results are reviewed and a clinical interpretation added to clinical portal and usually communicated by letter as well. All antenatal treatment of Syphilis infection is managed at Sandyford services. It is important to check the maternal record when reviewing a neonate. Advice can be obtained from your local genito-urinary medicine team (see box 1).
Maternal treatment is very effective at preventing congenital syphilis if a full course is given early in the pregnancy. Adequate treatment is defined as a parenteral penicillin preparation given for the required duration for the stage of disease. Parenteral penicillin is very safe for the mother (expected anaphylaxis risk of 0-3 per 100,000). There is a possible increased risk of pre-term delivery when treating early symptomatic syphilis in later pregnancy, due to the Jarisch Herxheimer reaction.
The recommended treatment course should have been completed more than 30 days before delivery and a fall in the RPR titre should have been documented following treatment if this was detectable at diagnosis. N.B. if there is any doubt about whether satisfactory treatment has been completed the Genito-Urinary Medicine team in charge of the mother’s treatment should be consulted (call Sandyford as above).
Inadequate maternal treatment includes the following:
- Treatment for less than the required period of therapy (see above) with a parenteral penicillin preparation. N.B. If more than one day of therapy is missed the course is inadequate and must be recommenced.
- Treatment with a non-penicillin regimen
- Infant delivered <30 days after completion of the antibiotic course
- Maternal RPR titres do not respond (if positive at diagnosis)
- Risk of re-infection from untreated partner or recurrent clinical signs
The mother’s HIV status must be determined (and result verified) as this has been shown to affect the course of syphilis infection both in the mother and neonate and make neonatal infection more likely.
The GUM team will classify the infant as ‘low risk’ or ‘high risk’ depending on the factors above and will communicate this to the GP, obstetric and neonatal teams using the template letter in appendix 1. Ideally, this should also be documented on maternal clinical portal and badger record (under specialist review).
If mother has had a false positive syphilis result or has been confirmed to have previously treated syphilis, the infant needs no further examination above routine and needs no serology (bloods) performed at birth.
All infants (low risk and high risk) whose mother has a true positive serological test for syphilis in this pregnancy need to be reviewed by the paediatrician shortly after delivery. Paediatrics need not attend delivery unless there are other indications. A detailed clinical evaluation is essential to look for signs of congenital syphilis as described above, recognising that two-thirds of infected infants will be asymptomatic.
All infants (low risk and high risk) should have syphilis serology performed on infant serum (not cord blood) for TP Syphilis IgM (specific IgM suggests congenital infection as fetus can produce IgM from 24 weeks gestation) and RPR – this requires 2ml of blood in EDTA tube. These should be accompanied by a maternal venous bloods sample for comparison (for IgM and RPR).
High risk infants
Infants born to mothers with primary, secondary or early latent phase maternal disease are at high risk in the following circumstances:
Neonate:
- Signs of congenital syphilis (see above)
- Infant TP Syphilis IgM test is positive, together with corroborative history, clinical signs
- Infant has positive dark ground microscopy (see below)
- Infant has positive T pallidum PCR test (see below) together with corroborative history, clinical signs
Maternal factors - these will be highlighted in birth plan from GUM (appendix 1):
- High maternal RPR titres e.g. a titre of 1:16 or greater
- Inadequate course of maternal treatment as defined above
- Mothers with symptoms of primary syphilis shortly before delivery irrespective of the serological results.
These infants need the following investigations:
- FBC,U+E, LFTs
- HIV antibody if not known from maternal booking bloods.
- Lumbar puncture for CSF WCC, protein, RPR, TPPA (For RPR and TPPA: CSF fluid into white topped virology tube)
- Long bone X-rays for osteochondritis and periostitis
- Chest X-ray for cardiomegaly
- Cranial U/S scan
- Ophthalmology assessment for interstitial keratitis
- Audiology for 8th nerve deafness
If baby is symptomatic on examination, also perform:
- T pallidum polymerase chain reaction (PCR) test – This test is done on any secretion or fluid from skin or oral lesions and fluid should be put into the white topped virology tube - discuss with the laboratory regarding sampling requirement prior to sending.
- Dark ground microscopy (DGM) – this is a test of fluid from a lesion on the skin. Fluid needs to be immediately placed on a slide and requires immediate interpretation so If this is required, discuss with the laboratory regarding sampling technique.
When samples are sent to the lab for TP Syphilis Antibody and RPR, the result can be interpreted as follows:
- TP Syphilis IgM: This is a direct antibody to the syphilis spirochaete and is positive in early infection and falls slowly (>2years). This test as reported as positive or negative. It does not cross the placenta so is a good marker for congenital syphilis infection if positive in neonate. A positive test indicates a need for treatment.
- The ‘IgM ratio’ is a supplement to this result and gives an indication to how recent the syphilis infection was. This is not important in management.
- RPR: (Rapid Plasma Reagin test) to non-treponemal (indirect) antibodies. This test detects biomarkers given off by cells damaged by the syphilis spirochaete. This reflects current disease activity and falls in response to adequate treatment. This test is reported as a titre. An RPR positive in ‘neat serum’ indicates a weakly positive test before dilution. If the test remains positive with dilution, this indicates a more convincingly positive test. If the RPR is positive at a dilution >4 fold compared to the mother (e.g. the mother is positive at 1:4 and the baby at 1:16), then this is a significantly positive test and indicates a requirement for treatment.
- TPPA: (Treponema Pallidum Particle Agglutination test): A specific treponemal antibody. The exact titre doesn’t really matter.
- TP-syphilis antibody (IgG): This is a direct antibody to the syphilis spirochete. The IgG will remain positive for life in anyone who has ever had syphilis infection, even after adequate treatment. This is not usually checked in the neonatal period.
(see flowchart below for interpretation)
A diagnosis of congenital syphilis is confirmed:
- If the infant’s serum is TP Syphilis IgM positive and/or
- There is a sustained elevation (two samples - the original screening sample and, if the original is positive, a repeat) showing a four-fold or greater difference of RPR titre above that of the mother (e.g mother RPR 1:4 and infant RPR 1:16 or greater).
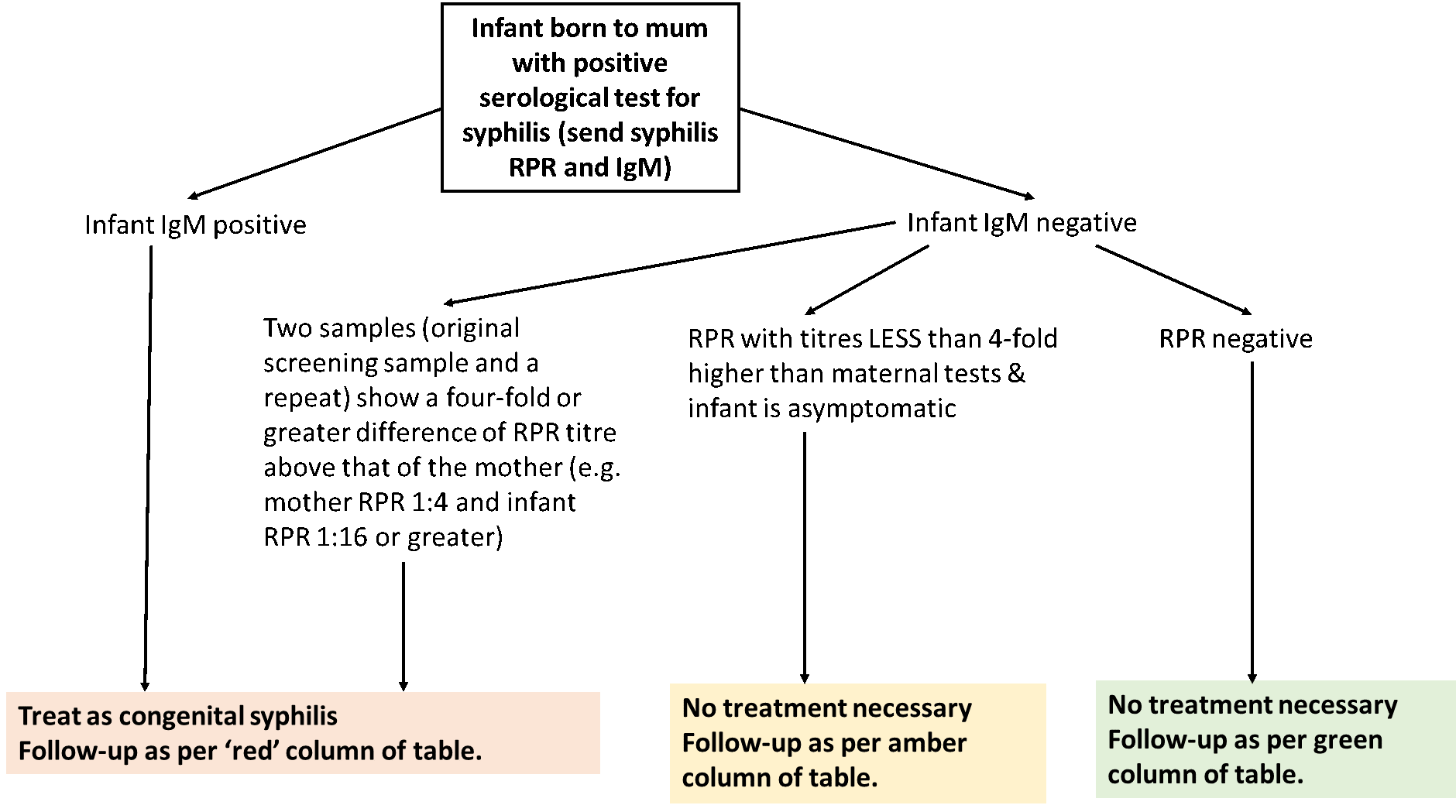
Treat all symptomatic infants, and all infants meeting the criteria of a serological diagnosis of syphilis (see flowchart above) with a full 10 day course of IV Benzylpenicillin. All infants commence on 50mg/kg/dose twice daily increasing to 50mg/kg/dose three times a day for term infants once >7days old.
High Risk Infants or those diagnosed with congenital syphilis infection
Follow up for high risk infants is essential at 3, 6 and 12 months or until RPR is negative, to ensure adequate treatment or absence of vertical infection. Negative RPR at 6 months excludes congenital syphilis. If the RPR does not fall or increases then repeat treatment with the above course is necessary. Successful treatment is defined as a 4 fold fall in RPR titres by 3 months following treatment and RPR negative at one year.
Those infants in whom CSF was indicative of neurosyphilis will also require repeat examination of CSF at six months of age. If CSF RPR is not negative after six months then a further course of treatment is indicated and a repeat CSF should be tested in a further 6 months.
Low Risk Infants
Low risk infants are defined above. These infants need serological tests for syphilis as above, performed shortly after delivery. No treatment is required for this group; however, serology should be repeated at 3, 6 and 12 months or until all tests become negative. Neonatal RPR should be negative by 6 months of age.
Summary of Follow-up Serological tests Required
|
Age |
Infants treated for congenital syphilis at birth |
Infant not treated for syphilis and RPR <4x mother’s and IgM negative at birth |
Infant not treated for syphilis and RPR and IgM negative at birth
|
|
1 month |
RPR TP Syphilis IgM |
|
|
|
3 months |
RPR TP Syphilis IgM |
RPR TP Syphilis IgM |
RPR TP Syphilis IgM If negative: discharge If positive: Repeat at 6 months |
|
6 months |
RPR |
RPR If negative: discharge If positive: repeat at 12 months |
RPR If negative: discharge If positive: discuss with GUM/ ID team. |
|
12 months |
RPR Discharge if RPR has achieved sustained 4x drop from peak level. If RPR remains higher, discuss with GUM/ ID team. |
RPR If negative: discharge If positive: discuss with GUM/ ID team. |
|
All siblings to new born infant should be assessed and screening for congenital syphilis infection. Serological testing can be arranged via the RHC infectious diseases team (on Dect Phone 84939 or through RHC Switchboard) or your local general paediatrics team.
- Hurtig et al. Syphilis in pregnant women and their children in the UK BMJ 1998;317:1617-9
- Guidelines for the management of early and late syphilis and guidelines on diagnosing congenital syphilis can be found at British Association for Sexual Health & HIV
- American Center for Disease Control (CDC) guidelines - Congenital syphilis
- Teaching Files: Syphilis Neonatology on the Web
- Health Protection Scotland. Syphilis.
- Greenall, J. Early congenital syphilis in a premature baby. European journal of pediatrics, 2011. 170(5), pp. 667-669.
- Taylor FJ. Preventing congenital syphilis: A review of the current epidemiology, screening, and treatment options. Infectious Diseases in Clinical Practice, 2013, 21(3), pp. 149-154.
- Galvao TF. Safety of benzathine penicillin for preventing congenital syphilis: a systematic review. PLoS ONE [Electronic Resource], 2013. 8(2), pp. e56463.
- Kingston M et al. UK national guidelines on the management of syphilis. 2015. International Journal of STD & AIDS; 0(0) 1–26; DOI: 10.1177/0956462415624059.
- Health Protection Scotland. Syphilis in Scotland 2018: an update. National Services Scotland.
- Public Health England. Addressing the increase in syphilis in England: an action plan. June 2019.
Last reviewed: 07 September 2020
Next review: 01 September 2023
Author(s): Dr Andrew MacLaren
Co-Author(s): Other professionals Consulted: Dr Becky Metcalfe – Consultant in Sexual Health and HIV Medicine, NHS GGC; June Grant – Neonatal Pharmacist, PRM; Dr Conor Doherty – Consultant in Paediatric Infectious Diseases
Approved By: West of Scotland Neonatology Managed Clinical Network