
Infant spinal anaesthesia, a guide
exp date isn't null, but text field is
Objectives
This is a guide / aide memoire for staff preparing for spinal anaesthesia in neonates & infants in theatre at RHC Glasgow.
Scope
Please note other departments use different equipment & set-up for lumbar puncture in a similar patient group.
Audience
Anaesthetists / Anaesthetic assistants at RHC Glasgow.
Further information please contact: jocelyn.erskine@ggc.scot.nhs.uk or graham.bell@ggc.scot.nhs.uk or the Duty anaesthetist 84842
Preterm, chronic lung disease, congenital heart disease and airway anomalies.
<5kg ideal, 5-8kg challenging but achievable. No specific upper age limit.
(after discussing the appropriateness of the technique with the surgeon)
Failure rate when you’re starting is about 1-in-10 to 1-in-30 when you’re good!
All the usual complications. Aseptic meningitis has been reported. Most major complications remain unreported (but possible).
Early apnoea rate greatly reduced compared to GA, late apnoeas are less common and seem to be due to patient (not anaesthetic) factors & there is no difference in incidence compared with GA.
Early evidence of limited developmental consequences related to total anaesthesia exposure in early life, these concerns persist on a google search but we should not use them to promote spinal anaesthesia use in patients.
Spinal anaesthesia does, however, result in favourable haemodynamics compared to GA.
- They need to be ready to start immediately (ie. Scrubbed in theatre whilst you are doing the spinal)
- The spinal will reliably last 45 mins but this can be extended to over an hour (and occasionally longer) with a caudal +/- clonidine additive
- The operating conditions are slightly different but this is ok!
- Choose a fast one to start with…
- Standard fasting advice
- EMLA covering both spinal and caudal injection sites

2. Anaesthetic equipment
- Ensure all equipment and machines checked
- Standard monitoring equipment inc rectal temp probe
- Set up for conversion to GA if required (face mask, circuit, laryngoscope, ETT ready)
- Emergency and GA induction drugs prepared
- Underbody FAWD
- 24% Sucrose ampules ready (can also use expressed breast milk)
- Identify the ‘baby holder’ (not another anaesthetist!)
- Diathermy pad ready to apply once regional block completed (can avoid inadvertent high block on raising the legs)
- Dummy (use patients’ own if possible, may need a premature one if <2.5kg)
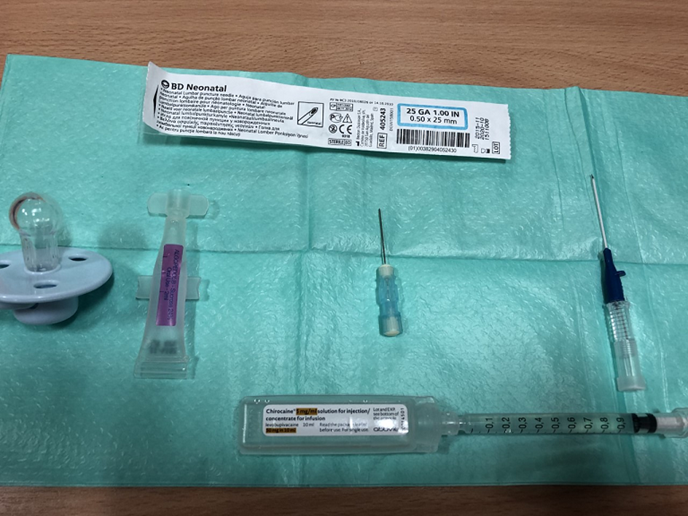
- Sucrose/EBM
- Spinal needles (we use 25G Neonatal Whitacre needles, Sprottes = 40mm are available)
- 5% chlorhexidine spray
- 5% Levobupivocaine (heavy can be used but difference in duration of block/spread is minimal, plain is our standard)
- Standard 22G caudal needle (Abbocath)
- Sterile saline
- Full sterile pack and trolley
- 2 sterile plasters or Dermabond®
- Consider other equipment to aid positioning e.g. warm towels to wrap baby (place in warming cabinet), right-angled anaesthetic bar.
- Patient directly into theatre
- Establish IV access if not already cannulated. Consider need for IV maintenance fluids as reducing lines attached can be advantageous.
- Consider nasal cannula for O2 or Air, especially in apnoea prone neonates
- Give atropine 5-10mcg/kg in preterms and all patients under 2.5kg. Can be given orally on ward preoperatively. Offsets bradycardia which can occur on onset of the sympathetic blockade.
- Calculate the spinal and caudal doses and ensure these are visible once scrubbed
- SURGEONS aware and scrubbing immediately after you so… ready
- POSITION POSITION POSITION. This is the most important factor in determining success! Lateral or supine is personal preference, both work.

SUPINE: Assistant stabilises baby from axilla to pelvic brim.


LATERAL: Assistant stabilises the head, other hand under the flexed knees and ‘curls’ the baby. Beware the risk of airway obstruction.
- Ensure the position is optimal BEFORE you scrub.
- If lateral position: put a little head up tilt on the bed
- EMLA removed and 2 sprays of 0.5% chlorhexidine (allowed to air dry)
- Have sucrose to administer just prior to needle insertion (by another individual, not the baby holder)
- Clear drapes allow everyone to see what they need to

Ensure the drape extends to include the sacral hiatus but no further- aim to keep any unexpected fluids on the ‘dirty’ side.

SPINAL ANAESTHESIA
- Dose: 1mg/kg levobupivocaine = 0.2mls/kg 0.5% levobupivocaine. Never less than 0.5mls.
- Add clonidine? Advice is on the departmental shared drive.
- Level: L3/4 to L5/S1 feel for the best space
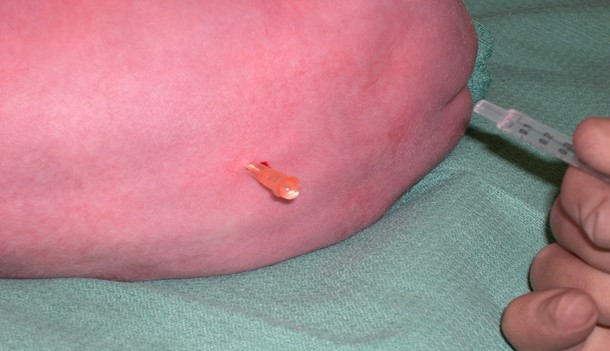
- It is a ‘feel’ so difficult to describe.
Top tips:
2 clicks & you’re in.
It’s deeper than you expect & almost never <10mm
Staying in the midline is everything
If you don’t get CSF back when you expect it then withdraw, don’t advance, & withdraw 1mm at a time
Bloody taps often clear to bloodstained CSF
Onset of the block in premmies is near instant but can take up to 10 minutes in a 3 month old
- When you’re in give half your dose immediately, then check aspirate (or disconnect) before second dose to allow repositioning of the needle if negative.
- If you’re not convinced about the spinal – pause for 5 minutes (a full 5 minutes) before doing the caudal so you can re-assess the spinal & you have the dose allowance to repeat if necessary
- Do not persist indefinitely, set yourself a reasonable number of attempts/time limit before cutting losses and proceeding with GA.
Once spinal sited proceed with caudal. This is optional but does appear to increase the density and duration of the block.
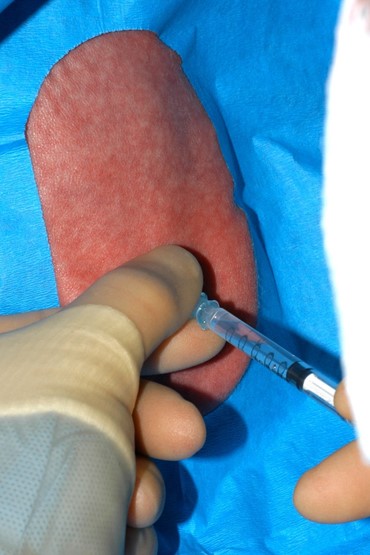
CAUDAL ANAESTHESIA
- Dose: 1.5mg/kg levobupivacaine = 0.3mls/kg 0.5% levobupivocaine diluted up to a sensible volume for the patient i.e. 0.75 – 1ml/kg total volume.
- Dilute with sterile saline
- Response to caudal needle often a good indicator of spinal efficacy
- SLOWER injection than normal… risk of a higher spinal block
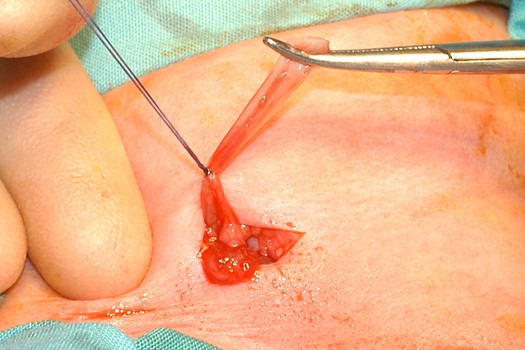
- Simple dressings OK but some smaller babies leak CSF from the lumbar puncture site & these should be sealed with Dermabond or a similar glue, this makes a mess but it’s microbiologically sound.
THEN
- SHOUT to surgeons if not immediately behind you to get ready to start
- Remove drapes
- Apply diathermy pad to back
- Turn patient supine
- Move monitoring to lower limbs
- Roll under hips if required (lift entire patient up in air to avoid block ascent)
- Shield patient from operative lights
- Position patient: aim to secure arms to reduce surgical interference, either arms wrapped in a towel or suspended loosely from right-angled bar.


Non-restrictive arm suspension
KNIFE TO SKIN
- You should have a good idea of whether the block is working already by the tone of the lower limbs
- Surgeons routinely do a ‘pinch test’ with toothed forceps. There should be no response (keeping in mind the baby may still be a little unsettled at this point due to new position etc). Make sure you are convinced before they start.
ENVIRONMENT
- Warm
- Dark
- Human contact can help
- Sucrose (usually just for initial period)
- May require additional O2 but this is not routine
- Sedation does occur with the spinal alone. Presumed mechanism is diminished afferent conduction to RAS. The patient will often sleep.

- Beware of vagal stimuli e.g. visceral traction leading to bradycardia, wriggling/discomfort
Being prepared is everything
Issues that occur:
- Inadequate block: as mentioned, spinal can be repeated if concerned at insertion time (provided caudal not already given)
- If persistent concerns convert to GA early. Not worth the stress on the patient or anyone else especially when establishing practice
- High block: head up tilt, sit baby up if appropriate. It may fall quickly if just inserted and institute these measures. If not, proceed with emergency management.
- Bloody tap. Common. Can clear to CSF so be patient. As mentioned above, withdraw 1mm at a time if not clearing and continually assess for appearance of CSF.
- Post op CSF leak. Minimise this with dressings/Dermabond®. Can still occur. Monitor and seek microbiology/neurosurgical advice.
- LA toxicity manage as per AAGBI guidelines. Management of severe local anaesthetic toxicity | Association of Anaesthetists
- Transfer to recovery (risk of early apnoeas is significantly reduced but not absent)
- Standard is to maintain 24hrs of SpO2 monitoring if <60wks post conceptual age.
- Can feed immediately
Many of these patients may be returning to NICU for ongoing care/transfer back to base hospital.
However, there may be patients outwith the NICU setting who are eligible for same day discharge. The decision to discharge should be at the discretion of the anaesthetist but factors to consider are:
- >60 weeks PCA (post conceptual age) for ex-preterm
- Weight >5kg
- No recent anaemia
- Adequate feeding re-established
- Comfortable
We are aware of the impending implementation of NR Fit equipment. We do not yet have the equipment available in RHC but updated photos will be obtained and uploaded as soon as we do.
Last reviewed: 12 July 2023
Next review: 31 July 2026
Author(s): Jocelyn Erskine, Graham Bell
Version: 1
Author Email(s): jocelyn.erskine@ggc.scot.nhs.uk
Approved By: Paediatric Anaesthetic Department Consultants