
Hypoglycaemia : term infants
exp date isn't null, but text field is
Objectives
Screening and management of hypoglycaemia in term infants in the first 48 hours of life.
This document and complementary flow charts details the criteria for screening and the subsequent management term infants at risk of hypoglycaemia during the first 48 hours of life. These infants may have impaired metabolic adaptation, and be potentially at risk of neurological damage when their blood glucose levels fall. They therefore require prompt and appropriate intervention.
This guideline is applicable to all Midwifery, Nursing and Medical staff caring for the newborn in The West of Scotland neonatal MCN and is cognisant of recent recommendations contained within the BAPM Framework for Practice, “Identification and management of neonatal hypoglycaemia in the full term infant, October 2017”1. Staff should be familiar with guidelines for the management of persistent or refractory hypoglycaemia which are separate to this document. All the advice regarding feeding and fluids within this document assume that there are no other medical issues. Where this is not the case individualised care plans will be required.
The importance of parents as partners in care is reinforced throughout this guidance which includes a parent information leaflet (Appendix) which explains why their baby is receiving extra monitoring for blood glucose levels and how to raise concerns about their baby’s feeding pattern or well being.
The definition of neonatal hypoglycaemia remains controversial1 2 as the neonate has the unique ability to utilise alternative fuels such as ketone bodies and lactate to sustain brain metabolism within the first days of life3. A recent consensus defined neonatal hypoglycaemia as a plasma glucose concentration of 2.5mmol/l or less.
It is important to note that these thresholds are raised to 3.0mmol/L in infants with suspected hyperinsulinism4 in the first 48hours.
3 groups of babies merit medical attention:
- Babies with risk factors for hypoglycaemia
- Babies with symptoms or signs of hypoglycaemia
- Babies with persistent or refractory hypoglycaemia - see WoS Guideline for Persistent or Refractory Hypoglycaemia
|
Signs and Symptoms of Hypoglycaemia in the Neonate Hypoglycaemia may present in a number of ways within the first 48 hours of life. These include;
This list is not exhaustive. Medical review should be obtained for any generally unwell infant as these symptoms may warrant further investigation and consideration of other causes including sepsis |
The normal breastfed baby may feed very infrequently or be reluctant to feed in the first 48 hours and small volumes of hand expressed colostrum are usually sufficient5. The importance of early expressing in the hours immediately after birth needs to be highlighted to staff and mothers. Supplementary feeds in these babies are unnecessary and can potentially undermine the confidence of the breastfeeding mother and may interfere with the normal metabolic adaptive responses that occur in the first few postnatal days6.
Neonatal review and initiation of blood glucose measurements should only be necessary in such babies if they are unduly sleepy or hypotonic or if there are other signs of clinical illness. Abnormal feeding behaviour as described below should prompt full clinical assessment and consideration of blood glucose measurement
A baby at significant risk of hypoglycaemia, or who has symptoms which may be secondary to hypoglycaemia, should be screened with regular monitoring of the capillary glucose concentrations.
Near patient testing devices tend to be less accurate in the lower range, especially < 2.0mmol/l7and therefore all low values (≤2.6mmol/L) require confirmation using blood gas analysis as this is considered the gold standard for measuring blood glucose.
Hand held glucometers should meet ISO standards (ISO15197:2013) and have CE marking as described in the BAPM Framework. If a handheld glucometer is used, low levels must be confirmed using an accurate method as cot-side monitors may be inaccurate in the lower ranges and require checking using a True Blood Glucose (TBG) to guide therapy A TBG can be obtained by sending a formal laboratory sample but significant delays can occur in obtaining a result, alternatively a TBG can also be obtained from a blood gas analyser, where available, as these are equally reliable8. All units must ensure they have readily accessible methods for accurate measurement of a TBG . Each unit must be aware of the characteristics of any near patient testing device used in their hospital.
|
Local Arrangements for Confirming Blood Glucose <2.6mmol/L GG&C - GG&C Maternity and Neonatal units use the Precision Exceed Pro meter©. For this device glucose values 2.6 - 3.0mmol/l may prove to be <2.6mmol/l when a TBG is obtained from a blood gas machine or laboratory testing. Therefore a TBG should be obtained for:
|
If normal adaptive metabolic and endocrine responses to extra-uterine life are absent or sub-optimal then babies are at increased risk of developing clinically significant hypoglycaemia.
The mainstay of management in this group is the prevention of hypoglycaemia by feeding early and regularly and keeping the baby warm.
Infants at risk of hypoglycaemia should be nursed with their mother in the postnatal ward unless there is a specific medical reason for admission to the neonatal unit.
Risk Factors for Hypoglycaemia
- Intrauterine growth restriction in term infants i.e ≥ 37+0 weeks (<2nd centile for sex and gestation)
- Infants less than 37 weeks gestation i.e. up to 36+6 weeks gestation regardless of weight centile – See separate WoS Guideline - Hypoglycaemia: Preterm Infants
- Maternal diabetes – Including both insulin dependent and gestational diabetes
- Macrosomic babies –Babies who weigh ≥ 4.5 kg
- Infants of mothers taking B blockers (labetalol, propranolol or atenolol) in the 3rd trimester and/or at the time of delivery including a single dose prior to delivery –
- Hypothermia - Inadvertent or therapeutic temperature ≤36.50 C persisting despite measures to treat
- Hypoxia – Babies who required prolonged resuscitation ( > 10 minutes)or with a cord pH <7.1 and/or BE > -12
|
Gestational Age (weeks) |
Boys Weight (Kg) |
Girls Weight (Kg) |
|
37 |
2.1 |
2.0 |
|
38 |
2.3 |
2.2 |
|
39 |
2.5 |
2.45 |
|
40 |
2.65 |
2.6 |
|
41 |
2.8 |
2.75 |
|
42 |
2.9 |
2.85 |
Birth weight gestational age thresholds for second centile in Kg by sex
(if birth weight is less than the defined threshold by sex and gestation of birth in weeks baby requires monitoring)
- Identify babies at risk of clinically significant hypoglycaemia at birth and commence a hypoglycaemia/NEWS monitoring chart in labour ward. All babies should be risk assessed for criteria for hypoglycaemia monitoring and/or NEWS monitoring prior to leaving a labour ward environment. Begin care as per flowchart A
- Aim to prevent hypoglycaemia
- Keep the baby warm - dry the baby well at birth, cover the baby whilst receiving skin to skin contact, put a hat on and avoid bathing until the temperature is stable and a warm environment is assured. This is likely to be after 24 hours of age. When dressing the baby, ensure that clothing is warmed first. Utilise skin-to-skin to warm the baby whenever needed.
- Skin to skin and the first feed – it is vital that this baby has the opportunity to have uninterrupted skin contact immediately after the birth (including instrumental and caesarean birth). The baby should have the full “magical hour” episode.
Do not assist the baby to feed too early before it is ready to attach correctly and feed effectively. Ideally the first feed should commence within the first 60 minutes. Assist the mother to recognise feeding cues (rapid eye movements under the eye lids, mouth and tongue movements, body movements and sounds, sucking on a fist).
If the baby has not feed by 90 minutes after the birth or is reluctant to feed follow reluctant feeder guidance LINK then start hand expressing and give the colostrum to the baby.
For women who wish to formula feed give 10-15ml/kg 3 hourly. - Blood glucose monitoring and clinical surveillance – The first blood glucose should be taken prior to the second feed usually at around 2-4 hours old9 10. Check the baby’s temperature, tone and respiratory rate at least 3 hourly to coincide with blood glucose measurements. Ensure that the baby is alert and normally responsive for their age and gestation. If the baby is unwell or has clinical signs of hypoglycaemia check a blood glucose immediately and alert the Neonatal Team urgently.
- Encourage effective feeding – Following the second feed, continue to offer lots of feeding opportunities, at least 3hly until blood glucose measurements have been > 2.5mmol on two consecutive occasions. Reinforce feeding cues; teach hand expressing and biological nurturing techniques to the mother early on as these will be essential for the “at risk” baby who needs to feed more often than those who are not at risk. Continue feeding support until mother and midwife are satisfied that effective feeding is established.
- Keep the baby warm - dry the baby well at birth, cover the baby whilst receiving skin to skin contact, put a hat on and avoid bathing until the temperature is stable and a warm environment is assured. This is likely to be after 24 hours of age. When dressing the baby, ensure that clothing is warmed first. Utilise skin-to-skin to warm the baby whenever needed.
- Screen capillary blood samples for hypoglycaemia immediately prior to each feed (3 hourly) using a cot-side testing device. Aim to maintain a pre-feed blood glucose of ≥2.5 mmol/l**. If blood glucose values <2.6 mmol/l are obtained follow the management pathways as per flowcharts B and C dependent on the additional presence of clinical signs of hypoglycaemia.
- **In some units, after careful consideration, a threshold pf > 2.0mmol/l has been deemed appropriate in line with BAPM guidance. All Health Care Professionals must ensure knowledge of local agreements of glucose threshold and clinical pathways. In NHS GG&C the threshold is to maintain a pre-feed glucose ≥2.5 mmol/l. Box for local arrangements
- Discontinue monitoring when blood glucose concentrations have been > 2.5 mmol/l on two consecutive occasions at least 3 hours apart. Observe feeding in hospital for a further 24 hours ensuring it is effective while remaining vigilant for the signs of hypoglycaemia. If signs of hypoglycaemia develop or there are concerns about feeding discuss with medical staff and consider taking a further blood glucose.
- After discontinuing regular glucose monitoring, continue feeding input
- If the baby is alert and keen to waken and feed, then promote responsive feeding.
- If the baby is still a bit sleepy, continue to waken and proactively offer feeds.
- Do not transfer babies with risk factors for impaired metabolic adaptation and hypoglycaemia to community care for at least 24 hours until you are satisfied that the baby is maintaining blood glucose levels and feeding well.
Blood Glucose >2.5mmol/l
- after two acceptable consecutive blood glucose measurements and a satisfactory feeding assessment provided there are no other clinical concerns, discharge is appropriate.
- If breastfeeding ensure at least 1 recorded breast feeding assessment utilising local/BFI tool prior to transfer home.
- Remaining vigilant for the signs of hypoglycaemia. If signs of hypoglycaemia develop or there are concerns about feeding discuss with medical staff and consider taking a further blood glucose.
|
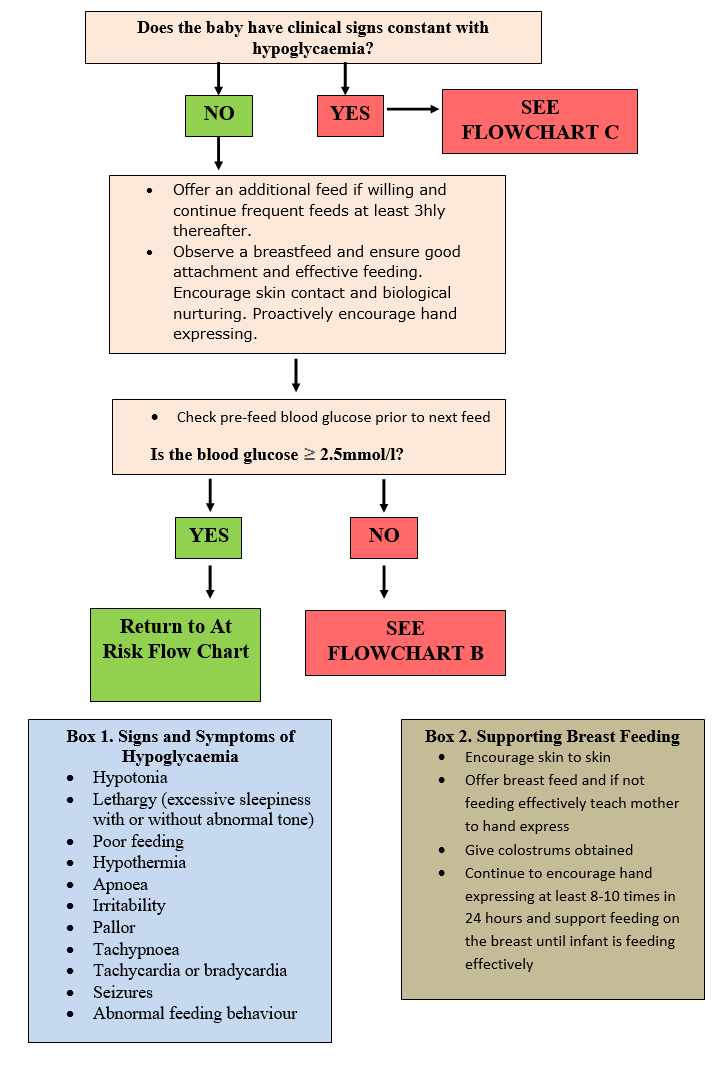
Green Zone/Flowchart A - Pre-Feed Glucose 2.0-2.5mmol and NO abnormal clinical signs |
- Offer an additional feed if willing and continue frequent feeds at least 3hly thereafter.
- Observe a breastfeed and ensure good attachment and effective feeding. Encourage skin contact and biological nurturing. Proactively encourage hand expressing.
- If two consecutive measurements fall within the Green Zone - -→ Treat as Amber Pathway
|
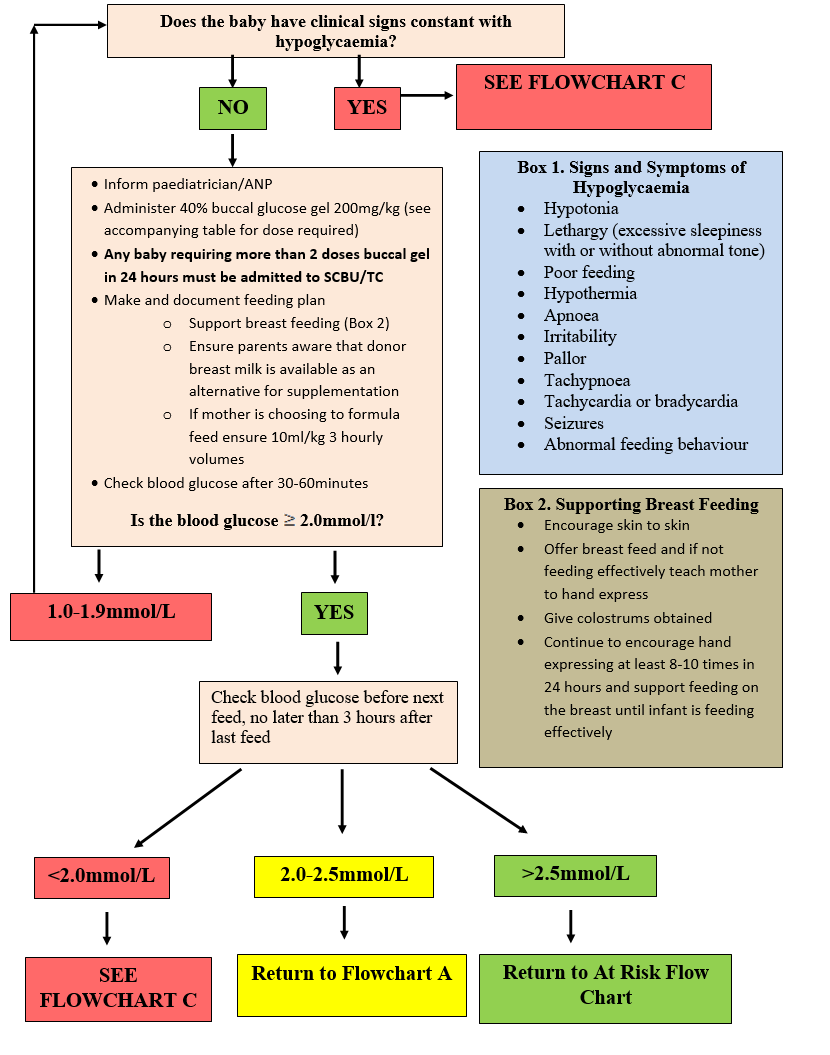
Amber Zone/Flowchart B – Glucose 1.0 - 1.9 mmol/l - Supplement and Paediatric review |
- Inform Neonatal Doctor/ANP
- Administer a dose of 40% buccal glucose 200mg/kg (see table below for dose dependent on weight and directions for administration) this must be given in conjunction with making and documenting a detailed feeding plan.
- Check blood glucose 30-60 minutes after administration of buccal gel.
- If glucose remains 1.0-1.9mmol on post gel blood glucose check administer second dose of buccal gel. The baby be reviewed by a member of the neonatal team as soon as is practical.
- Repeat blood glucose after 30-60 mins.
- All doses of buccal gel MUST be administered in conjunction with a careful review of feeding including a clear feeding plan which ensures adequate volumes are being administered:
- If breast feeding support breast feeding
- Encourage skin to skin
- Offer breast feed and if not feeding effectively teach mother to hand express and use breast pump
- Give colostrum obtained
- Continue to encourage hand expressing at least 8-10 X/24 hrs and support feeding on the breast until the infant is feeding effectively.
- Ensure families are aware that donor breast milk is available as an option for supplementation.
- If formula fed ensure adequate feed volumes are being given (at least 10ml/kg) in 3 hourly volumes.
- Check blood glucose before next feed, no later than 3 hours after feed irrespective of the blood glucose result 30-60 minutes obtained post gel as theoretically a delayed drop in blood glucose may occur.
- If hypoglycaemia of <2.0mmol/L persists after two doses of dextrose gel or the infant becomes symptomatic manage as per red zone/Flowchart C
If baby is not feeding adequately consider admission to SCBU/TC for NG feeding.
|
Red Zone/Flowchart C - Pre-Feed Glucose <1.0mmol/l OR Clinical Signs Consistent with Hypoglycaemia at a higher blood glucose concentration |
- Inform Neonatal Team
- Management will include appropriate investigations (see Investigations for Persistent Hypoglycaemia below) at time of hypoglycaemia for persistent hypoglycaemia as described below
- Continue to establish breastfeeding unless the baby is too unwell to feed
- Obtain IV access
- Give 2.5ml/kg 10% glucose bolus IV
- If unable to obtain IV access immediately give either
- 40% glucose gel 200mg/kg
OR
- Glucagon 200micrograms/kg IM dependent on unit preference and availability
- Followed by IV glucose as above when IV access available
- Start infusion of IV 10% glucose at 90ml/kg/day
- Recheck blood glucose 30 minutes after above
- Blood glucose <2.0mmol/l or abnormal clinical signs
- Further 2.5ml/kg 10% glucose bolus
- Increase glucose delivery rate as per flowchart (link)
- Consider temporary cessation of enteral feeds
- Recheck blood glucose after 30 minutes
- Blood glucose 2.0-2.5mmol/l and no abnormal clinical signs
- Increase glucose delivery rate as per flowchart
- Continue feeding if no contraindication
- Recheck blood glucose after 30 minutes
- Blood glucose >2.5mmol/l
- Slowly wean IV infusion
- Monitor blood glucose every 3 hours while establishing full enteral feeds
- Maintain blood glucose above 2.5mmol/l or 3.0mmol/l if hyperinsulinism suspected/confirmed.
- Continue to monitor blood glucose pre feeds ( 3hrly) for at least 24 hours after full enteral feeds established .
- Blood glucose <2.0mmol/l or abnormal clinical signs
Transient hypoglycaemia defined as ONE measurement of 1.0 to 1.9mmol/l within the first 48 hours of life in an infant with no abnormal signs who is feeding effectively DOES NOT require such investigations.
A new born with persistent (3 or more) episodes of blood glucose < 2.0 mmol/l within the first 48 hours of life or < 1.0 mmol/l at any time should undergo consideration of investigations for persistent hypoglycaemia (See WoS Guideline for persistent or Refractory Hypoglycaemia). These investigations must be taken during the period of hypoglycaemia.
In addition to metabolic investigations in infants with persistent hypoglycaemia consider screening and treating for sepsis
In most babies, hypoglycaemia is transient, lasting only a few days, and may be managed with moderate increases in glucose intake. It is very important to identify those infants with refractory hypoglycaemia (hypoglycaemia persisting despite a glucose intake of > 10mg/kg/min of glucose) or persistent hypoglycaemia (hypoglycaemia persisting for more than 2-3 days), as the aetiology is likely to be different. Infants with refractory hypoglycaemia are uncommon, and should be discussed with the attending Consultant. Refractory hypoglycaemia carries a very significant risk of long term neurological problems and metabolic disease will need to be excluded.

For babies who are on a combination of different fluids +/- milk there is a handy online calculator at http://nicutools.org/
Indications
- Blood glucose 1.0-1.9 mmol/l as component of feeding plan when following Flowchart B
NB should have no abnormal clinical signs
- Blood glucose <2.0mmol/l if delay in obtaining IV access
- >37 weeks
- <48 hours of age
Dose
- 200mg/kg glucose gel (0.5ml/kg of 40% glucose gel)
|
Weight of Baby (Kg) |
Volume of Gel (ml) |
|
1.5-1.99 |
1.0 |
|
2.0-2.99 |
1.5 |
|
3.0-3.99 |
2.0 |
|
4.0-4.99 |
2.5 |
|
5.0-5.99 |
3.0 |
|
6.0-6.99 |
3.5 |
Method of administration
- Draw up 40% glucose gel using a 2.5 or 5ml enteral syringe
- Dry oral mucosa with gauze
- Gently apply half of the dose to inner cheek and massage into mucosa using gloved fingers and then repeat on the inner cheek on the other side
- Offer a feed preferably breast milk immediately after administration
A Neonatal Doctor/ANP must review all babies receiving a dose of buccal glucose gel and that they remain asymptomatic with no concerning clinical signs, review (Temp, RR, HR)
All doses of buccal gel MUST be given in line with the agreed pre-printed prescription and the date and time clearly documented on this as well as appropriate section of the NEWS chart
BG must be obtained within 30-60 minutes of any dose of buccal glucose gel to monitor response
If blood glucose remains 1.0-1.9 mmol/l give second dose of buccal gel.
Regardless of blood glucose measurement recorded 30-60 minutes post administration of buccal gel a repeat must be obtained no more than 3 hours later as theoretically a delayed drop in blood glucose may occur.
If >2 doses of buccal gel required within a 24 hour period requires SCBU/TC admission
Pre-feed Blood Glucose 2.0-2.5mmol/l and NO Abnormal Clinical Signs
Pre-feed Blood Glucose 1.0-1.9mmol/l and NO Abnormal Clinical Signs
Blood Glucose <1.0mmol/l and/or Clinical Signs with Hypoglycaemia

Last reviewed: 21 March 2023
Next review: 01 March 2026
Author(s): Dr Natalie Smee – Paediatric Trainee RHC; Dr Lesley Jackson – Neonatal Consultant RHC
Co-Author(s): Other Professionals consulted: Ms Gillian Bowker - Infant Feeding Advisor GG&C; Mrs Anisa Patel - Neonatal Pharmacist RHC; Mrs Lauren Williams - Neonatal Pharmacist RHC